Short case H.T.NO. :1701006131; N JOSHUA PAUL
25 YR OLD MALE WITH CHEST PAIN, VOMITINGS AND SOB
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box"



 2D ECHO DONE ON 8-2-23
2D ECHO DONE ON 8-2-23 BLOOD AND URINE INVESTIGATIONS
BLOOD AND URINE INVESTIGATIONS
A 25 YEAR OLD MALE WITH FEVER AND HEADACHE
Date of admission : 7-2-23
25/M painter by occupation who was apparently asymptomatic 9 years back,
Patient c/o blurring of vision for which he went to local hospital used medication but his blurring of vision(Rt>>Lt) wasn't subsided
In 2014 patient c/o severe weight loss approximately 10-12 kgs over a duration of 2 months. And having increased apetite, increased frequency of urination with these complaints he went to Local hospital and diagnosed with type 1 diabetes mellitus and since then he was started on Mixtard insulin 28U -x - 24U and since then he is on regular follow up.. His fbs used to be around 200-250 and ppbs around 250-300
Last HbA1c was 11.2 on feb 3rd
Now since 1 week patient came with c/o fever high grade associated with chills and rigors, Nausea, Vomitings , constipation
And c/o neck pain
No c/o chest pain palpitations , syncopal attacks
No meningeal signs
At presentation his grbs is 234 mg/dl with urine for ketones ++
Outside 24hr urine proteins 3920mg/day
On presentation his vitals are
Afebrile
BP - 110/80 mmhg
PR - 86bpm
Spo2 - 100 at RA
CVS - S1S2+
RS - normal vesicular breath sounds heard
On HAI infusion according to Algorithm 1
Not a k/c/o HTN / Asthma / CAV / CAD
Personal history :
Sleep: adequate
Appetite: normal
Diet: mixed
Bowel and bladder movements: normal
Addictions: none
Family history :
No similar complaints in family
General examination :
Patient Is conscious, coherent, cooperative moderately built and well nourished
pallor - Absent
icterus - Absent
clubbing - Absent
cyanosis - Absent
lymphadenopathy - Absent
Edema - Absent
Vitals:
TEMP-96.5 F
PR-82/MIN
RR-14/MIN
BP-110/70MMHG
SPO2-99% AT ROOM AIR
GRBS-197MG%.
Systemic examination :
CVS - S1S2 present, no murmur
RS - Bilateral air entry present, trachea central in position
CNS - Higher mental functions intact
P/A - Soft, non tender
Clinical images with investigations:
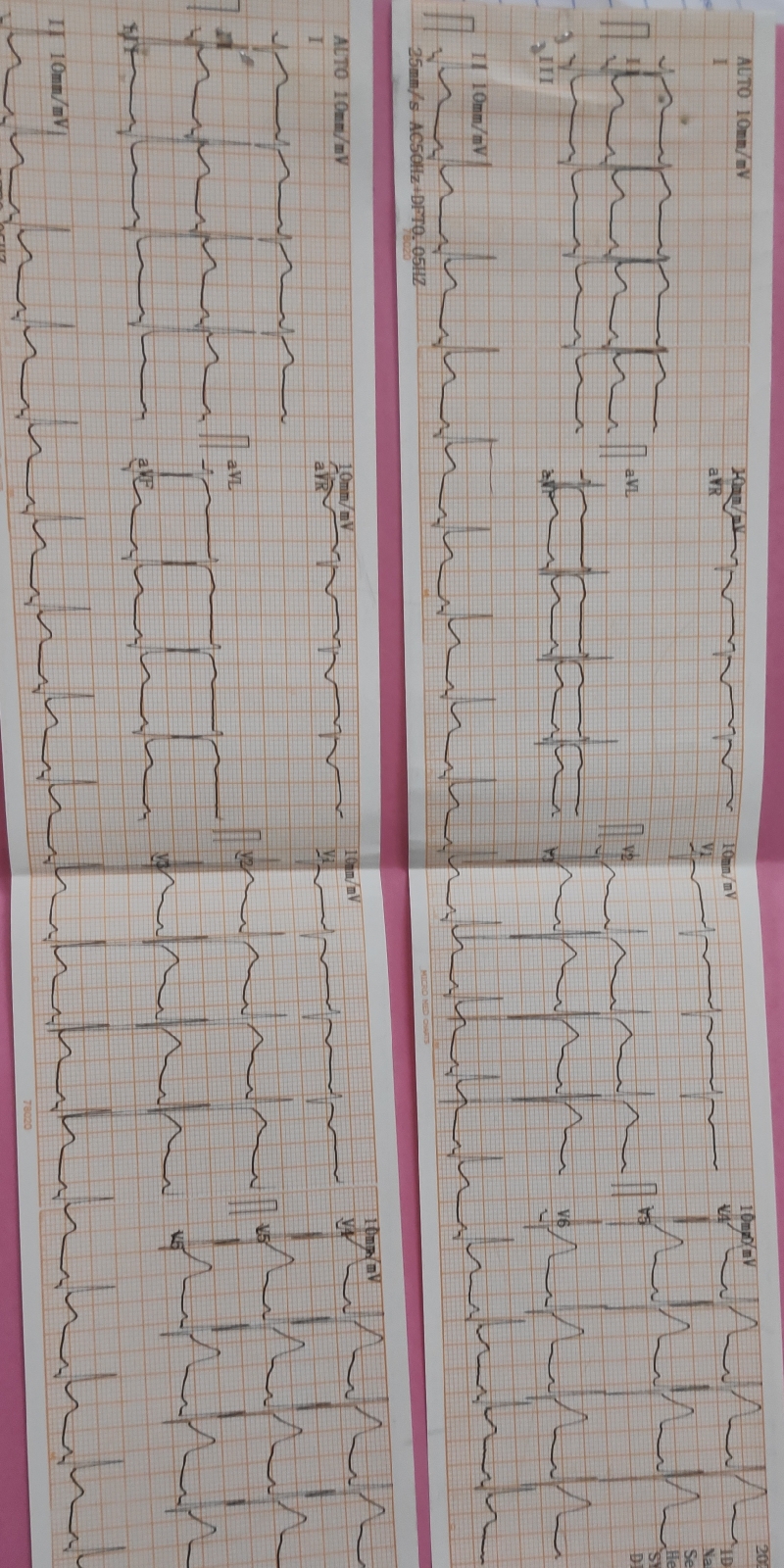
ECG DONE ON PRESENTATION 8-2-23

REPEAT ECG 8-2-23
 USG ABDOMEN DONE ON 8-2-23
USG ABDOMEN DONE ON 8-2-23
Diagnosis :
DIABETIC KETOACIDOSIS(RESOLVED) WITH OLD INFERIOR WALL MI WITH K/C/O TYPE I DM SINCE 9YRS WITH DIABETIC NEPHROPATHY
Treatment :
* IV FLUIDS NS@75ML/HR
5% DEXTROSE IF GRBS <= 250MG/DL
* HUMAN ACTRAPID INSULIN INFUSION ( 1ML +39 ML NS) @ 3ML/HR BASED ON GRBS
* TAB ECOSPRIN GOLD 75/75/10MG PO HS
* GRBS MONITORING HOURLY
* STRICT I/O CHARTING.
* VITALS MONITORING 2ND HRLY.



Comments
Post a Comment